

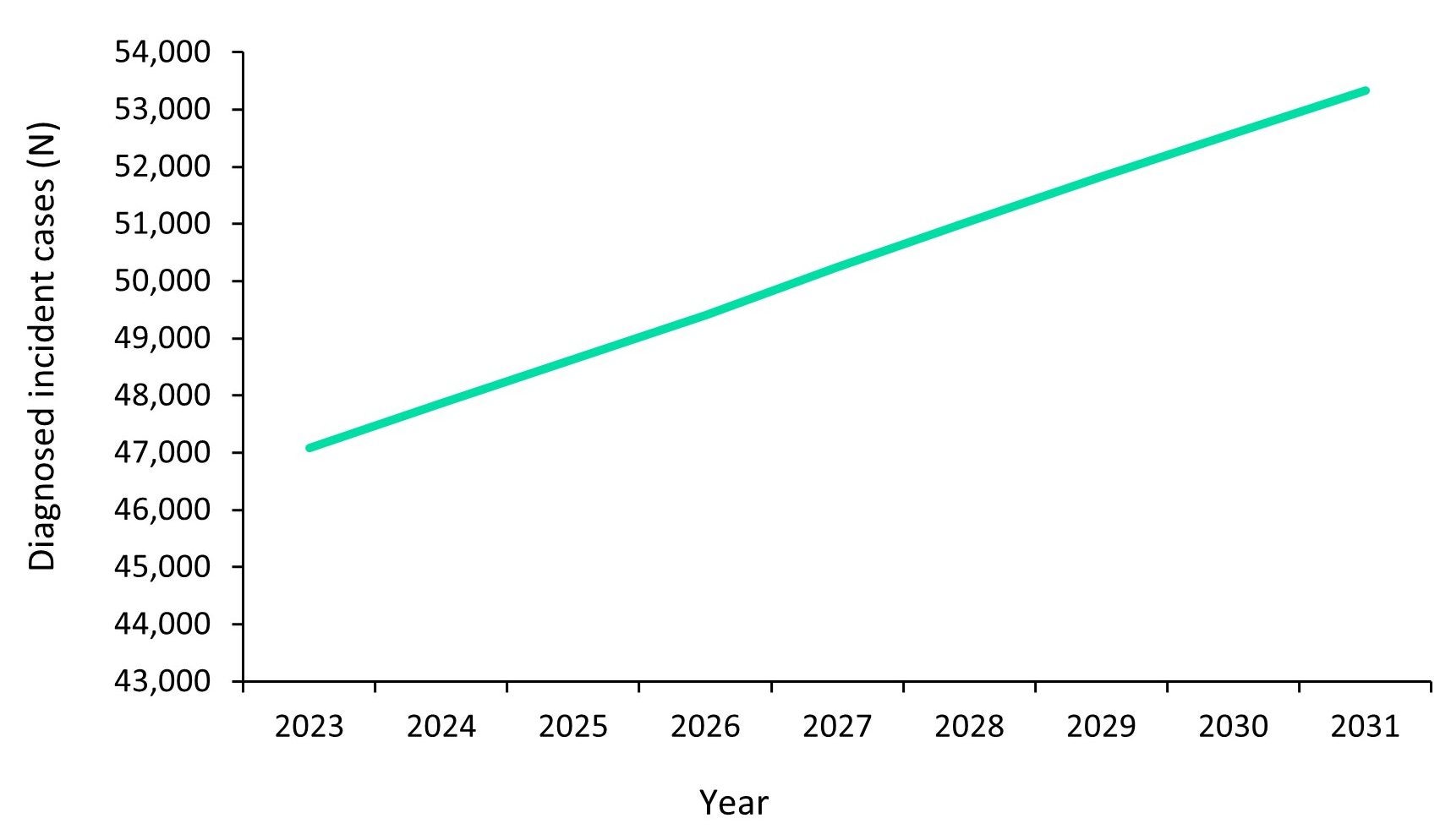
Source: GlobalData.
The Bowel Cancer Screening Programme (BCSP) was introduced in England in 2006 with the intention of lowering colorectal cancer (CRC) incidence and mortality. The program initially involved sending a biennial guaiac faecal occult blood test (gFOBT) to everyone aged 60 to 69 years; this age range was later extended to include 70 to 74-year-olds in 2010 to reflect the increasing life expectancy. CRC is the second most common cause of death in the UK; it has a long lag period of ten to 15 years from which an initial polyp develops into a cancerous tumour. Secondary prevention through screening programs such as BCSP can reduce the CRC mortality rate by identifying and removing precancerous lesions before they reach the advanced stage of the disease. The diagnosed incident cases of CRC in the UK alone are predicted to reach just over 42,000 by the end of 2023 and over 53,000 by the end of 2031 by GlobalData epidemiologists (Figure 1, above). However, the effectiveness of the BCSP in reducing the CRC incidence rate since its rollout in 2006 has not yet been quantified. So, Granger and colleagues conducted a 2023 population-based study published in Colorectal Disease, looking at the temporal trends in CRC incidence by tumour location, gender, and socioeconomic status from 2001 to 2017, and found that the screening program benefited men from deprived areas.
A total of 541,515 incident cases of CRC from 2001 to 2017 in people aged 60–74 years were identified using the National Cancer Registration and Analysis Service (NCRAS). Patient demographic data, tumour subtype (proximal and distal CRC), and stage at diagnosis were all available to the researchers.
The overall trend in CRC age-standardised incidence rates (ASIR) for both proximal and distal CRC was higher in men than women throughout the study period. The annual percentage change (APC) for proximal tumours in both genders remained relatively unchanged from 2001 to 2007, with men presenting an APC of 3.8% and women at 3.9%. However, since 2008, the ASIR in men has reduced considerably more than in women, with a negative APC of 2.1% and 1.1%, respectively. There was an increasing ASIR in men and women for distal tumours from 2001–2010 for men and 2001–2011 for women. Subsequent reductions in ASIR were more pronounced in men than women, with a negative APC of 6.8% and 3.6%, respectively; however, women sustained their APC more than men post-2014, with a negative APC of 3.6% and 0.3%, respectively. The ASIR of proximal tumours in the most deprived group was higher than the least deprived group for the whole study period, but those most deprived saw the most benefits from the BCSP and witnessed a statistically significant reduction in the ASIR of proximal tumours from 2008 onwards. Similar differences between the two socioeconomic groups were seen for ASIR of distal tumours; however, the magnitude of the difference in incidence rates was less over the course of the study period for the least deprived group.
Men benefited the most from the screening programme, even though the uptake was lower compared to women. The general increase in incidence after the initial introduction of BCSP can be explained by the identification of previously undiagnosed CRC cases. The subsequent decline in ASIR of CRC can then be explained by the identification of potentially cancerous lesions, which were then removed. The study highlighted groups that benefited the most from BCSP: men from deprived areas and those with distal tumours. This study has not only quantified the effectiveness of the BCSP but also provided helpful information for public health officials on the demographic that needs more encouragement for participation.



{kind=link}